Disease-Specific Comorbidity Clusters in COPD and Accelerated Aging

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Experimental Section
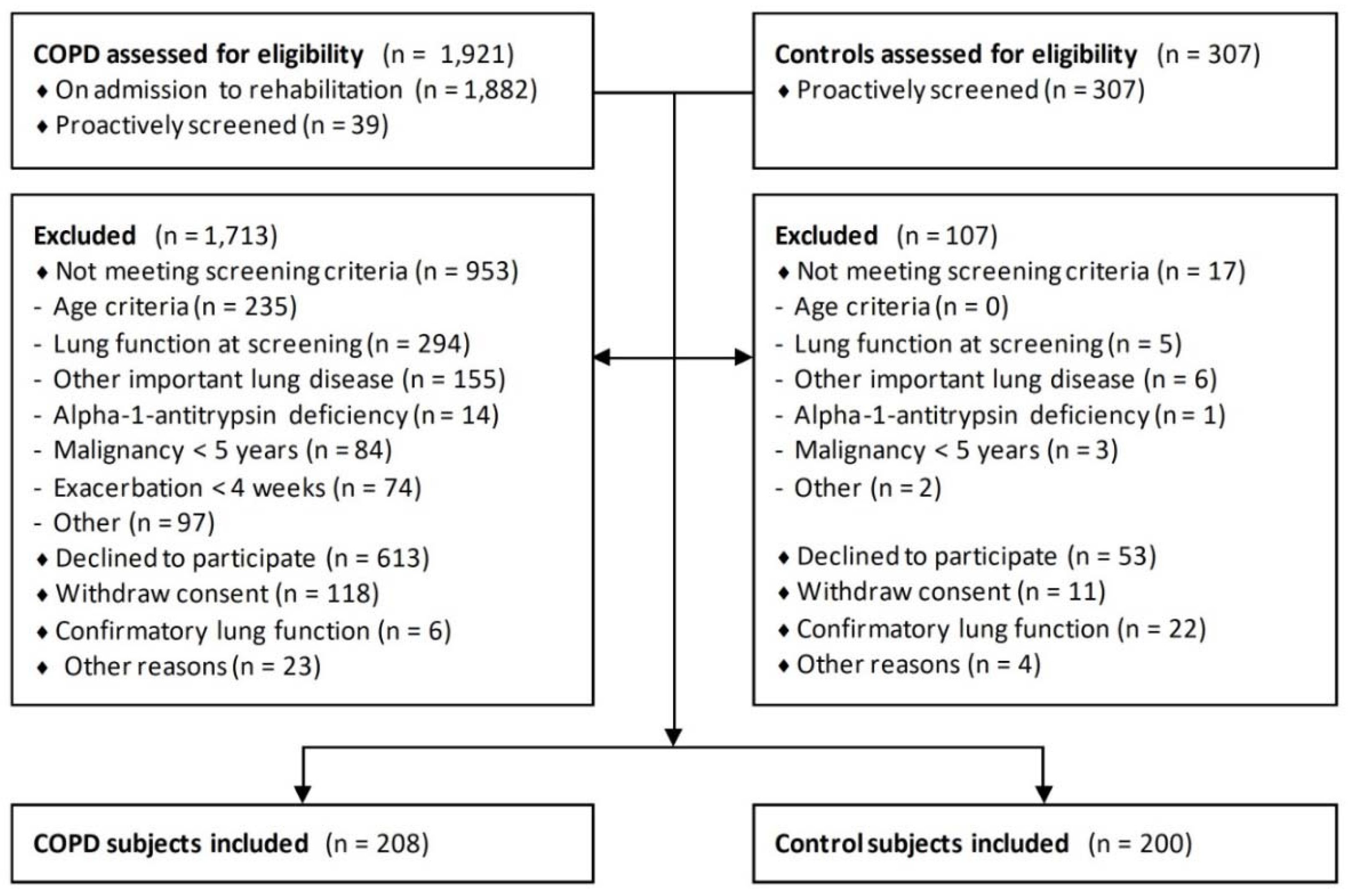
2.1. Study Design and Population
2.2. Assessments
2.3. Definitions
2.4. Statistical Analysis
3. Results
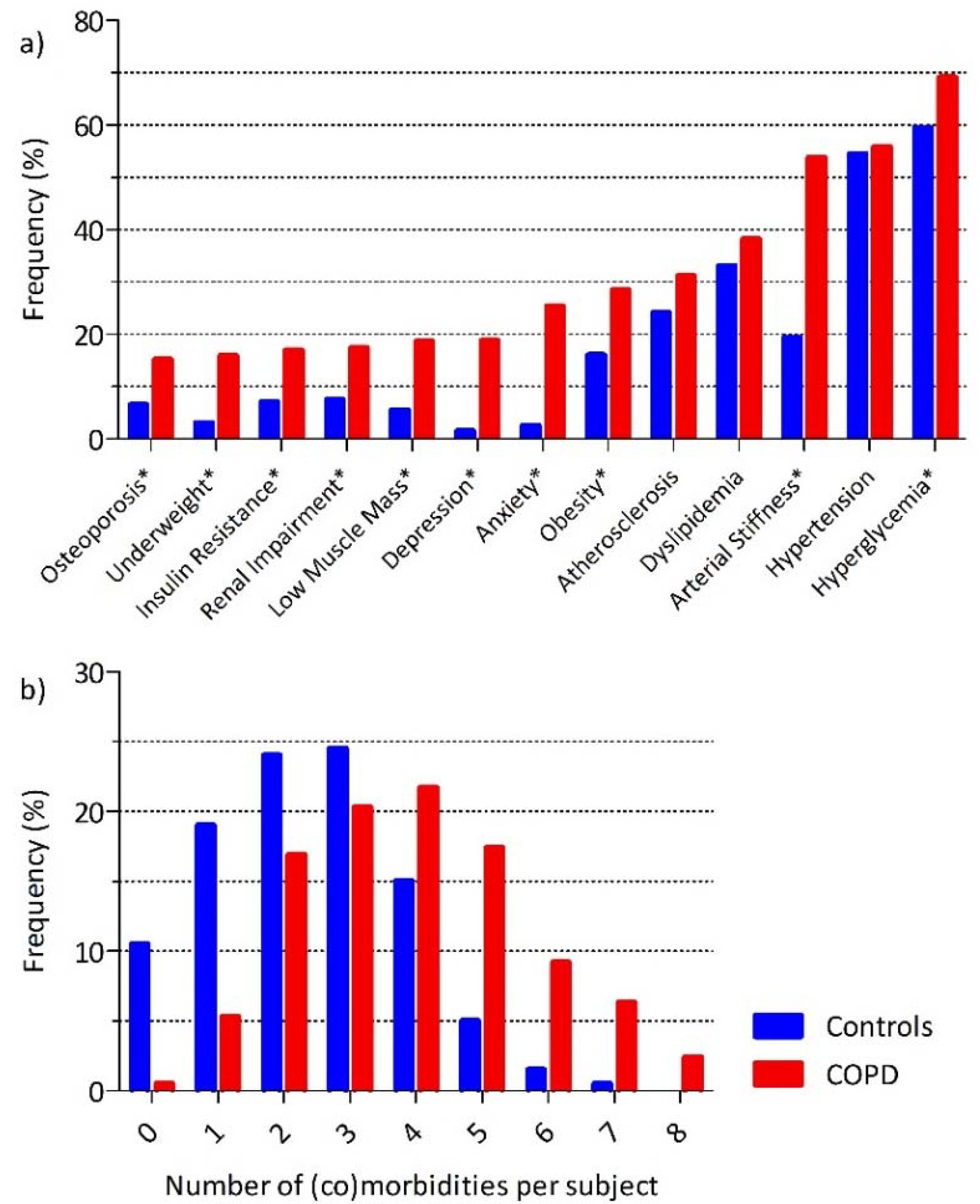
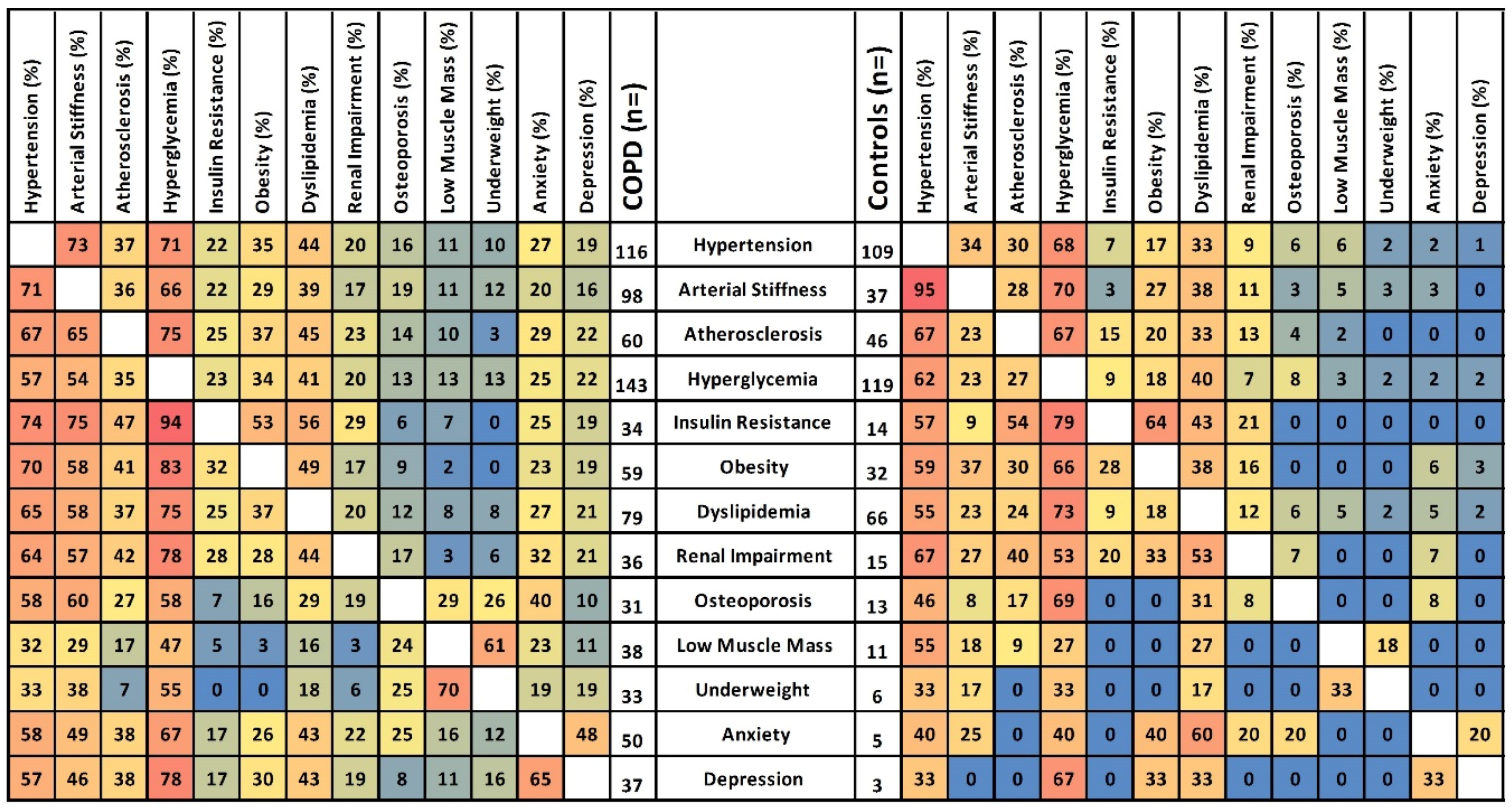
3.1. General Characteristics and (Co)Morbidities
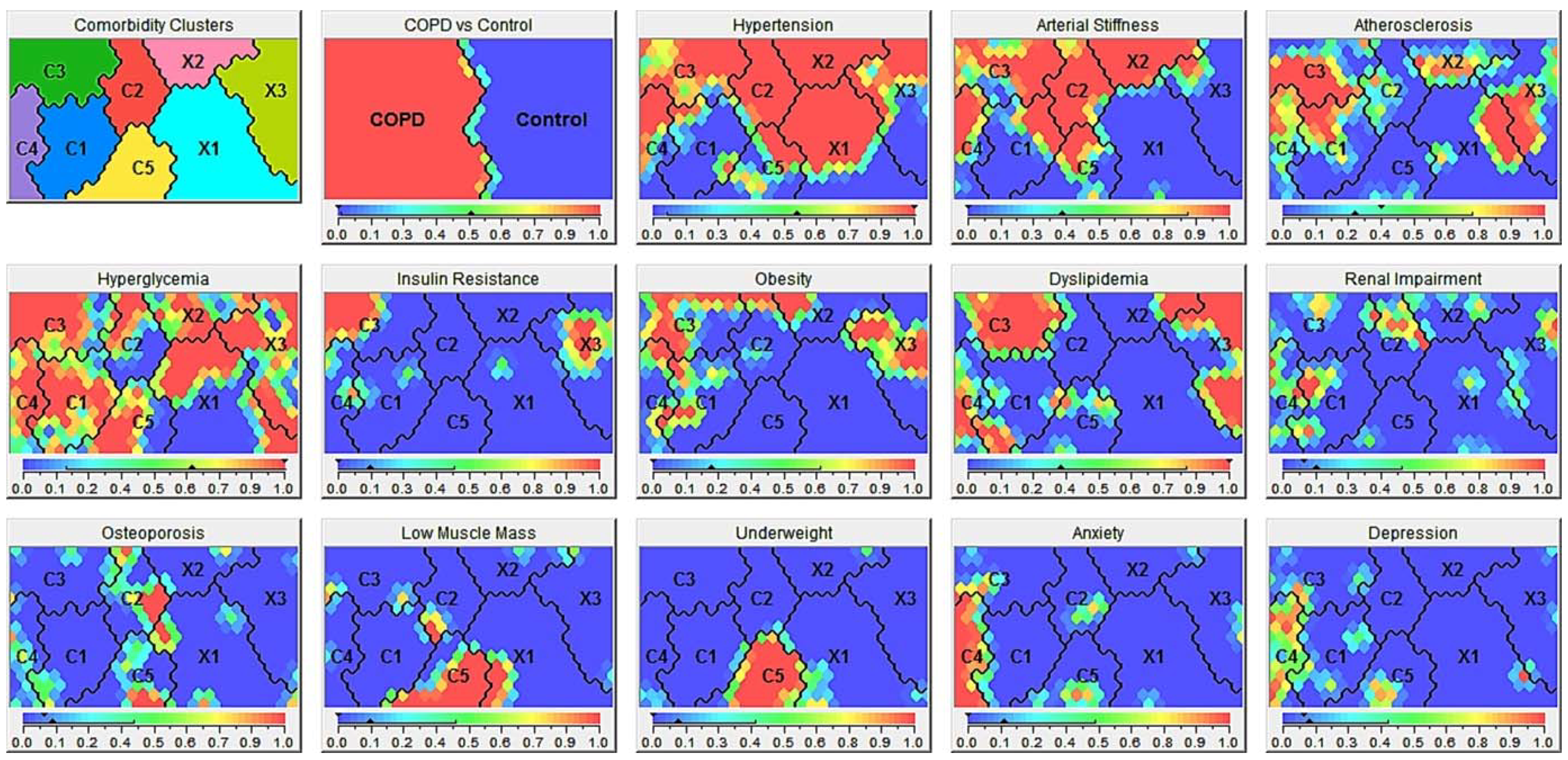
3.2. (Co)Morbidity Clusters
3.2.1. Comorbidity Clusters in COPD
3.2.2. (Co)Morbidity Clusters in Controls
3.2.3. Comparing (Co)Morbidity Clusters in COPD and Controls
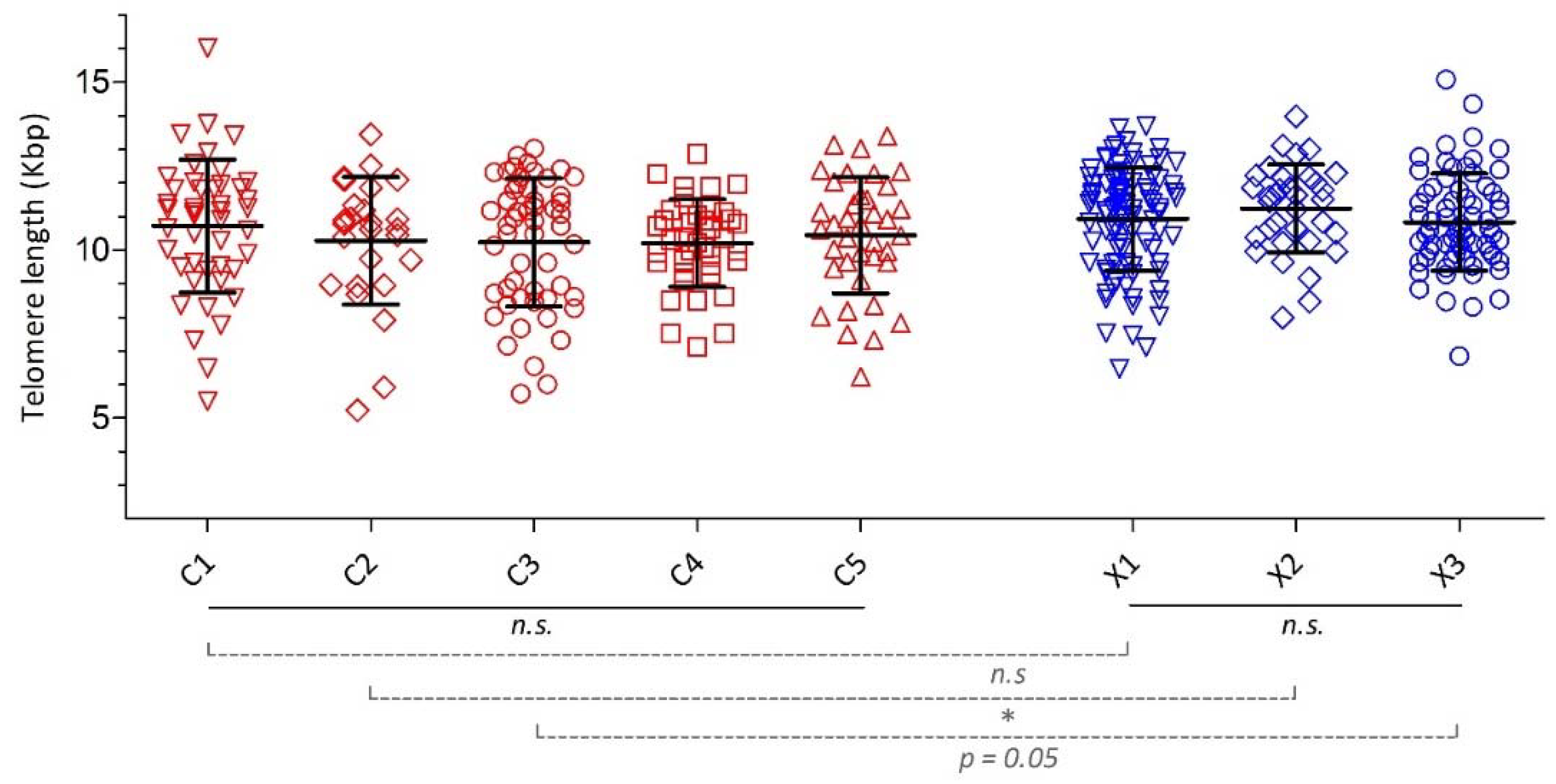
3.3. Telomere Length
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Subject Enrollment
Appendix A.2. Assessments
Appendix A.2.1. General Characteristics
Appendix A.2.2. Assessments of (Co)Morbidities
- Body mass index (BMI = body weight in kg/(height in m)2. Height was measured to the nearest 0.1 cm. Body weight was assessed to the nearest 0.1 kg after emptying the bladder and with the subjects standing barefoot and wearing light indoor clothing.
- Fat-free mass index (FFMI) = fat free mass in kg (=lean mass + bone mineral content by dual X-ray absorptiometry (DEXA) scan (Lunar Prodigy, GE Healthcare)) divided by (height in m)2 [33].
- Bone mineral density (BMD by DEXA scan) at the hip, lumbar spine, and whole body [34].
- Anxiety and depression were assessed by using the Hospital Anxiety and Depression Scale (HADS), a validated and reliable measurement instrument used widely in medically ill patients to screen for clinically relevant symptoms of anxiety and/or depression [35]. The HADS is a self-administered questionnaire, consisting of 14 questions. The HADS is divided into an anxiety subscale (HADS-A) and a depression subscale (HADS-D), both containing seven items. Total scores for each subscale can range from 0 (optimal) to 21 (worst) points.
- Pulse wave velocity (PWV) assessment methods were similar in the CIROCO and ICE Age studies and have been published before [36]. Radial artery waveforms were recorded with a high-fidelity micromanometer (Millar Instruments, Houston, TX, USA). The APWV was measured by recording ECG-gated carotid and femoral artery waveforms. The Sphygmocor systems software helped to assure the quality of the pulse wave measurement. A detailed screen showed 10 s of recorded and analyzed waveforms which can be examined to assess overall consistency of the waveforms. In addition, a detailed report helped to interpret the consistency of the waveforms during the 10-s measurement. Only when the pulse height and diastolic variation was less than 5%, the average pulse height was more than 100 units, the augmentation index was less than 50%, T1 was between 80 and 150 ms, and the overall “quality index” above 80 points, data were retained. After marking the exact location measurements, it was repeated three times for securing reproducibility. A measurement was accepted when it was reproducible three times with minimal variation as judged by the biomedical technologist. The retained APWV was the mean of the three measurements. Shortest distances from manubrium to the marked location on the femoral artery (via the navel) were measured. Wave transit time was calculated by the system software, using the R-wave of the simultaneously recording electrocardiography as reference frame. The APWV was determined by dividing the distance between the two recording sites by the wave transit time.
- Carotid intima-media thickness (c-IMT) was assessed using high-resolution B-mode ultrasound with a 10-MHz linear transducer (Art. LabEsoatePicus, Pie-medical Netherlands/Italy). The ultrasound device was connected to an acquisition modem with an automatic boundary detection system (Art.LabExoatePicus). Carotid IMT was thus quantified semi-automatically, reducing the interobserver variability [37]. With the patient in a supine position, measurements of the carotid IMT were performed throughout 10-mm segments across the bifurcation free of visual plaques. The probe was moved to obtain measurements of the left common carotid artery at 4 angles (180°, 150°, 120°, and 90°). For each measured segment, mean and maximum IMT values were acquired automatically throughout the 10-mm vessel length. The average of segmental maximum carotid values was determined as carotid IMT per patient.
- Peripheral systolic and diastolic blood pressure measurements were performed early in the morning after 15 min in a resting supine position. A small head pillow was accepted. Peripheral blood pressure was measured three times with intervals of 5 min.
- Laboratory analysis: A venous blood sample was collected in the fasted state. Serum, plasma, and peripheral blood mononuclear samples were stored at −80 °C prior to their analysis. Glucose, creatinine, high-density lipoprotein (HDL), and triglycerides were determined in all subjects. Fasting plasma glucose and serum insulin concentration were used to calculate the homeostasis model assessment method (HOMA index: fasting serum insulin (μU/mL) × fasting plasma glucose (mmol/L)/22.5), plasma creatinine concentration to calculate the estimated glomerular filtration rate (eGFR) using the simplified Modification of Diet in Renal Disease (MDRD) equation [38].
Appendix A.2.3. Telomere Length
Appendix A.3. Definitions
- COPD and grades of severity were classified according to the GOLD document [41].
- OBESITY was defined as a BMI equal to or above 30 kg/m2 according to the WHO international classification of BMI [42].
- HYPERGLYCEMIA was defined as fasting glucose level equal to or above 5.6 mmol/L according to the American Diabetes Association [43].
- INSULIN RESISTANCE. The homeostasis model assessment method (HOMA 1 IR index) is a simple and validated method to assess insulin sensitivity [44]. It is also an independent predictor of cardiovascular disease in patients with type 2 diabetes mellitus [45]. It was calculated as follows: HOMA index = fasting serum insulin (μU/mL) × fasting plasma glucose (mmol/L)/22.5. Cut-off values depended on geographic variation and gender, and defining a local population, percentile-based cut-off is recommended for the HOMA index and/or hyperinsulinemia [46,47]. Therefore, we used the 75th percentile of the HOMA 1 IR of the Hoorn study, a large Dutch cohort study in men and women aged 50 to 75 years was used to define insulin resistance [48]. We based the cut-off on the entire population of the Hoorn study without exclusion of patients with diabetes mellitus and/or prevalent cardiovascular disease and used separate values for males and females. These data were provided by personal communication with JM Dekker. Insulin resistance was defined as a HOMA 1 IR equal to or above 4.43 for males and 4.29 for females.
- DYSLIPIDEMIA was defined as a triglyceride level above 1.7 mmol/L or a HDL cholesterol level below 1.03 mmol/L in males or below 1.29 mmol/L in females [49].
- HYPERTENSION was defined as a systolic blood pressure equal to or above 140 mmHg or diastolic pressure equal to or above 90 mmHg, in line with the European Society of Hypertension (ESH)/European Society of Cardiology (ESC) guidelines [50].
- ARTERIAL STIFFNESS was defined as pulse wave velocity (PWV) > 10 m/s, as proposed by the expert consensus document of the Artery Society, the European Society of Hypertension Working Group on Vascular Structure and Function, and the European Network for Noninvasive Investigation of Large Arteries [51]. This value is at the upper part of the second quartile in the Framingham Heart Study and represents in this general population with a mean age of 63 years about 4% risk for a first major cardiovascular event within the next 8 years [52].
- ATHEROSCLEROSIS was defined as a maximal carotid intima media thickness (IMT) > 0.9 mm, which is according to the ESH/ESC guidelines compatible with subclinical organ damage [50].
- UNDERWEIGHT was defined as a BMI lower than 21 kg/m2. The purpose of a BMI cut-off point is to identify within a population, the proportion of people with a high risk of an undesirable health state. Hence, a BMI lower than 21 kg/m2, which has shown to be independently associated with one-year mortality in COPD, is an appropriate cut-off [42,53].
- LOW MUSCLE MASS was defined as a fat free mass index (FFMI) less than 17.05 kg/m2 for men or less than 14.62 kg/m2 for women, according to the lowest 10th percentile of the general population as reported in the Copenhagen City Heart Study [54], which is also supported by the Nutritional assessment and therapy in COPD statement of the European Respiratory Society statement [33].
- OSTEOPOROSIS was assessed by DEXA scanning and established if the lowest T score of the lumbar spine or hip was lower than −2.5 for females and lower than −2.8 for males, according to Dutch guidelines [55].
- RENAL IMPAIRMENT was defined as an eGFR less than 60 mL/min/1.73 m2, which was estimated, using the simplified Modification of Diet in Renal Disease (MDRD) equation [38], corresponding with stage 3 chronic kidney disease according to the National Kidney Foundation Kidney Disease Outcome Quality Initiative (NKF KDOQI) guidelines [56].
- ANXIETY was assessed, using the Hospital Anxiety and Depression Scale (HADS). A score equal to or greater than 10 points on the items related to anxiety, was considered to indicate symptoms of anxiety [35].
- DEPRESSION was also assessed, using the HADS. A score equal to or greater than 10 points on the items related to depression, was considered to indicate symptoms of depression [35].
Appendix A.4. Baseline Data

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COPD | All Controls | |
|---|---|---|
| Plasma glucose level, mmol/L | 6.2 ± 1.6 | 5.9 ± 0.9 1 |
| Systolic blood pressure, mmHg | 145 ± 22 | 143 ± 20 |
| Diastolic blood pressure, mmHg | 84 ± 9 | 84 ± 10 |
| Pulse wave velocity, m/s | 10.6 ± 2.7 | 8.8 ± 2.2 1 |
| Plasma triglyceride level, mmol/L | 1.5 ± 0.8 | 1.4 ± 1.0 |
| Plasma HDL level, mmol/L | 1.6 ± 0.5 | 1.6 ± 0.5 |
| cIMT, µm | 836 ± 181 | 800 ± 156 1 |
| HOMA index | 3.4 ± 6.0 | 2.0 ± 1.4 1 |
| eGFR, mL/min/1.73 m2 | 73.6 ± 15.8 | 77.6 ± 13.6 1 |
| BMI, kg/m2 | 26.9 ± 5.4 | 26.9 ± 3.4 |
| FFMI, kg/m2 | 17.6 ± 2.6 | 18.1 ± 3.1 |
| Lowest T score | −1.7 ± 1.0 | −0.9 ± 1.1 1 |
| HADS anxiety, score | 6.6 ± 4.2 | 3.5 ± 2.7 1 |
| HADS depression, score | 6.0 ± 3.9 | 2.0 ± 2.2 1 |
Appendix A.5. Telomere Length
| C1 | C2 | C3 | C4 | C5 | X1 | X2 | X3 | |
|---|---|---|---|---|---|---|---|---|
| Subjects, n (%) | 46 (22%) | 27 (13%) | 56 (27%) | 40 (19%) | 39 (19%) | 97 (49%) | 34 (17%) | 69 (35%) |
| Telomere length, kbp | 10.71 ± 1.99 | 10.27 ± 1.90 | 10.22 ± 1.90 | 10.20 ± 1.31 | 10.44 ± 1.73 | 10.92 ± 1.54 | 11.23 ± 1.32 1 | 10.82 ± 1.45 2 |
| Crude OR | Age Adj. OR | Age–Sex Adj. OR | |
|---|---|---|---|
| C1 | 1.15 (0.95–1.40) | 1.15 (0.94–1.39) | 1.15 (0.95–1.40) |
| C2 | 0.96 (0..77–1.21) | 0.99 (0.78–1.25) | 0.99 (0.78–1.26) |
| C3 | 0.94 (0.79–1.12) | 0.95 (0.80–1.13) | 0.95 (0.80–1.14) |
| C4 | 0.94 (0.77–1.14) | 0.93 (0.76–1.12) | 0.91 (0.75–1.11) |
| C5 | 1.03 (0.84–1.25) | 1.01 (0.83–1.23) | 1.01 (0.82–1.23) |
| Crude OR | Age Adj. OR | Age–Sex Adj. OR | |
|---|---|---|---|
| X1 | 0.98 (0.81–1.19) | 0.99 (0.82–1.20) | 1.01 (0.83–1.23) |
| X2 | 1.19 (0.91–1.54) | 1.22 (0.91–1.63) | 1.21 (0.91–1.61) |
| X3 | 0.92 (0.75–1.12) | 0.92 (0.76–1.13) | 0.91 (0.74–1.11) |
References
- Agusti, A.G. COPD, a multicomponent disease: Implications for management. Respir. Med. 2005, 99, 670–682. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Eur. Respir. J. 2017. [Google Scholar] [CrossRef]
- Pinto, L.M.; Alghamdi, M.; Benedetti, A.; Zaihra, T.; Landry, T.; Bourbeau, J. Derivation and validation of clinical phenotypes for COPD: A systematic review. Respir. Res. 2015, 16, 50. [Google Scholar] [CrossRef] [PubMed]
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.; Gaffron, S.; van Empel, V.P.; Bruijnzeel, P.L.; Rutten, E.P.; Op ‘t Roodt, J.; Wouters, E.F.; Franssen, F.M. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2013, 187, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Clini, E.M.; Beghé, B.; Fabbri, L.M. Chronic Obstructive Pulmonary Disease Is Just One Component of the Complex Multimorbidities in Patients with COPD. Am. J. Respir. Crit. Care Med. 2013, 187, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Barnes, P.J. COPD as a disease of accelerated lung aging. Chest 2009, 135, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Savale, L.; Chaouat, A.; Bastuji-Garin, S.; Marcos, E.; Boyer, L.; Maitre, B.; Sarni, M.; Housset, B.; Weitzenblum, E.; Matrat, M.; et al. Shortened telomeres in circulating leukocytes of patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2009, 179, 566–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Mello, M.J.; Ross, S.A.; Briel, M.; Anand, S.S.; Gerstein, H.; Pare, G. Association between shortened leukocyte telomere length and cardiometabolic outcomes: Systematic review and meta-analysis. Circ. Cardiovasc. Genet. 2015, 8, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Casanova, C.; Marin, J.M.; Pinto-Plata, V.M.; de-Torres, J.P.; Zulueta, J.J.; Cabrera, C.; Zagaceta, J.; Sanchez-Salcedo, P.; Berto, J.; et al. COPD comorbidities network. Eur. Respir. J. 2015, 46, 640–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutten, E.P.A.; Gopal, P.; Wouters, E.F.M.; Franssen, F.M.E.; Hageman, G.J.; Vanfleteren, L.E.; Spruit, M.A.; Reynaert, N.L. VArious mechanistic pathways representing the aging process are altered in copd. Chest 2016, 149, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Sabit, R.; Bolton, C.E.; Edwards, P.H.; Pettit, R.J.; Evans, W.D.; McEniery, C.M.; Wilkinson, I.B.; Cockcroft, J.R.; Shale, D.J. Arterial stiffness and osteoporosis in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2007, 175, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Cabrera, C.; Casanova, C.; Marin, J.M.; Pinto-Plata, V.; de-Torres, J.P.; Zulueta, J.; Zagaceta, J.; Sanchez-Salcedo, P.; Berto, J. Comorbidity Distribution, Clinical Expression and Survival in COPD Patients with Different Body Mass Index. Chronic Obstr. Pulm. Dis. 2014, 1, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harik-Khan, R.I.; Fleg, J.L.; Wise, R.A. Body mass index and the risk of COPD. Chest 2002, 121, 370–376. [Google Scholar] [CrossRef]
- Aoshiba, K.; Nagai, A. Senescence Hypothesis for the Pathogenetic Mechanism of Chronic Obstructive Pulmonary Disease. Proc. Am. Thorac. Soc. 2009, 6, 596–601. [Google Scholar] [CrossRef]
- Tsuji, T.; Aoshiba, K.; Nagai, A. Alveolar cell senescence in patients with pulmonary emphysema. Am. J. Respir. Crit. Care Med. 2006, 174, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Alder, J.K.; Guo, N.; Kembou, F.; Parry, E.M.; Anderson, C.J.; Gorgy, A.I.; Walsh, M.F.; Sussan, T.; Biswal, S.; Mitzner, W.; et al. Telomere length is a determinant of emphysema susceptibility. Am. J. Respir. Crit. Care Med. 2011, 184, 904–912. [Google Scholar] [CrossRef] [PubMed]
- McAllister, D.A.; Maclay, J.D.; Mills, N.L.; Mair, G.; Miller, J.; Anderson, D.; Newby, D.E.; Murchison, J.T.; Macnee, W. Arterial Stiffness is Independently Associated with Emphysema Severity in Patients with COPD. Am. J. Respir. Crit. Care Med. 2007, 176, 1208–1214. [Google Scholar] [CrossRef]
- Benetos, A.; Okuda, K.; Lajemi, M.; Kimura, M.; Thomas, F.; Skurnick, J.; Labat, C.; Bean, K.; Aviv, A. Telomere length as an indicator of biological aging: The gender effect and relation with pulse pressure and pulse wave velocity. Hypertension 2001, 37, 381–385. [Google Scholar] [CrossRef]
- Coxson, H.O.; Dirksen, A.; Edwards, L.D.; Yates, J.C.; Agusti, A.; Bakke, P.; Calverley, P.M.; Celli, B.; Crim, C.; Duvoix, A.; et al. The presence and progression of emphysema in COPD as determined by CT scanning and biomarker expression: A prospective analysis from the ECLIPSE study. Lancet Respir. Med. 2013, 1, 129–136. [Google Scholar] [CrossRef]
- Cordoba-Lanus, E.; Cazorla-Rivero, S.; Espinoza-Jimenez, A.; de-Torres, J.P.; Pajares, M.J.; Aguirre-Jaime, A.; Celli, B.; Casanova, C. Telomere shortening and accelerated aging in COPD: Findings from the BODE cohort. Respir. Res. 2017, 18, 59. [Google Scholar] [CrossRef]
- Baty, F.; Putora, P.M.; Isenring, B.; Blum, T.; Brutsche, M. Comorbidities and burden of COPD: A population based case-control study. PLoS ONE 2013, 8, e63285. [Google Scholar] [CrossRef] [PubMed]
- Chubachi, S.; Sato, M.; Kameyama, N.; Tsutsumi, A.; Sasaki, M.; Tateno, H.; Nakamura, H.; Asano, K.; Betsuyaku, T. Identification of five clusters of comorbidities in a longitudinal Japanese chronic obstructive pulmonary disease cohort. Respir. Med. 2016, 117, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Maurer, J.; Rebbapragada, V.; Borson, S.; Goldstein, R.; Kunik, M.E.; Yohannes, A.M.; Hanania, N.A.; for the ACCP Workshop Panel on Anxiety and Depression in COPD. Anxiety and depression in COPD: Current understanding, unanswered questions, and research needs. Chest 2008, 134, 43S–56S. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Albrecht, E.; Sillanpaa, E.; Karrasch, S.; Alves, A.C.; Codd, V.; Hovatta, I.; Buxton, J.L.; Nelson, C.P.; Broer, L.; Hagg, S.; et al. Telomere length in circulating leukocytes is associated with lung function and disease. Eur. Respir. J. 2014, 43, 983–992. [Google Scholar] [CrossRef] [PubMed]
- Boyer, L.; Chouaïd, C.; Bastuji-Garin, S.; Marcos, E.; Margarit, L.; Le Corvoisier, P.; Vervoitte, L.; Hamidou, L.; Frih, L.; Audureau, E.; et al. Aging-Related Systemic Manifestations in COPD Patients and Cigarette Smokers. PLoS ONE 2015, 10, e0121539. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Otin, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The hallmarks of aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef]
- Fletcher, C.M.; Elmes, P.C.; Fairbairn, A.S.; Wood, C.H. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br. Med. J. 1959, 2, 257–266. [Google Scholar] [CrossRef]
- Hernandes, N.A.; Wouters, E.F.; Meijer, K.; Annegarn, J.; Pitta, F.; Spruit, M.A. Reproducibility of 6-minute walking test in patients with COPD. Eur. Respir. J. 2011, 38, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A self-complete measure of health status for chronic airflow limitation. The St. George’s Respiratory Questionnaire. Am. Rev. Respir. Dis. 1992, 145, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Schols, A.M.; Ferreira, I.M.; Franssen, F.M.; Gosker, H.R.; Janssens, W.; Muscaritoli, M.; Pison, C.; Rutten-van Molken, M.; Slinde, F.; Steiner, M.C.; et al. Nutritional assessment and therapy in COPD: A European Respiratory Society statement. Eur. Respir. J. 2014, 44, 1504–1520. [Google Scholar] [CrossRef] [PubMed]
- Graat-Verboom, L.; Spruit, M.A.; van den Borne, B.E.; Smeenk, F.W.; Wouters, E.F. Whole-Body versus Local DXA-Scan for the Diagnosis of Osteoporosis in COPD Patients. J. Osteoporos. 2010, 2010, 640878. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Vanfleteren, L.E.; Spruit, M.A.; Groenen, M.T.; Bruijnzeel, P.L.; Taib, Z.; Rutten, E.P.; Op ‘t Roodt, J.; Akkermans, M.A.; Wouters, E.F.; Franssen, F.M. Arterial stiffness in patients with COPD: The role of systemic inflammation and the effects of pulmonary rehabilitation. Eur. Respir. J. 2014, 43, 1306–1315. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.C.; Brands, P.J.; Hoeks, A.P. Automatic recognition of the common carotid artery in longitudinal ultrasound B-mode scans. Med. Image Anal. 2008, 12, 653–665. [Google Scholar] [CrossRef]
- Levey, A.S.; Greene, T.; Kusek, J.W.; Beck, G.J. A simplified equation to predict glomerular filtration rate from serum creatinine. J. Am. Soc. Nephrol. 2000, 11, 155A. [Google Scholar]
- Cawthon, R.M. Telomere length measurement by a novel monochrome multiplex quantitative PCR method. Nucleic Acids Res. 2009, 37, e21. [Google Scholar] [CrossRef]
- de Vos-Houben, J.M.; Ottenheim, N.R.; Kafatos, A.; Buijsse, B.; Hageman, G.J.; Kromhout, D.; Giltay, E.J. Telomere length, oxidative stress, and antioxidant status in elderly men in Zutphen and Crete. Mech. Ageing Dev. 2012, 133, 373–377. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S.; Agusti, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Consultation, W.E. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33, S62–S69. [Google Scholar] [CrossRef] [PubMed]
- Bonora, E.; Targher, G.; Alberiche, M.; Bonadonna, R.C.; Saggiani, F.; Zenere, M.B.; Monauni, T.; Muggeo, M. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: Studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care 2000, 23, 57–63. [Google Scholar] [CrossRef]
- Bonora, E.; Formentini, G.; Calcaterra, F.; Lombardi, S.; Marini, F.; Zenari, L.; Saggiani, F.; Poli, M.; Perbellini, S.; Raffaelli, A.; et al. HOMA-Estimated Insulin Resistance Is an Independent Predictor of Cardiovascular Disease in Type 2 Diabetic Subjects: Prospective data from the Verona Diabetes Complications Study. Diabetes Care 2002, 25, 1135–1141. [Google Scholar] [CrossRef] [Green Version]
- Gayoso-Diz, P.; Otero-Gonzalez, A.; Rodriguez-Alvarez, M.X.; Gude, F.; Garcia, F.; De Francisco, A.; Quintela, A.G. Insulin resistance (HOMA-IR) cut-off values and the metabolic syndrome in a general adult population: Effect of gender and age: EPIRCE cross-sectional study. BMC Endocr. Disord. 2013, 13, 47. [Google Scholar] [CrossRef]
- Balkau, B.; Charles, M.A.; Drivsholm, T.; Borch-Johnsen, K.; Wareham, N.; Yudkin, J.S.; Morris, R.; Zavaroni, I.; van Dam, R.; Feskins, E.; et al. Frequency of the WHO metabolic syndrome in European cohorts, and an alternative definition of an insulin resistance syndrome. Diabetes Metab. 2002, 28, 364–376. [Google Scholar]
- Dekker, J.M.; Girman, C.; Rhodes, T.; Nijpels, G.; Stehouwer, C.D.; Bouter, L.M.; Heine, R.J. Metabolic syndrome and 10-year cardiovascular disease risk in the Hoorn Study. Circulation 2005, 112, 666–673. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Mancia, G.; De Backer, G.; Dominiczak, A.; Cifkova, R.; Fagard, R.; Germano, G.; Grassi, G.; Heagerty, A.M.; Kjeldsen, S.E.; Laurent, S.; et al. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2007, 25, 1105–1187. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D.; et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, G.F.; Hwang, S.J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial stiffness and cardiovascular events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The Body-Mass Index, Airflow Obstruction, Dyspnea, and Exercise Capacity Index in Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Vestbo, J.; Prescott, E.; Almdal, T.; Dahl, M.; Nordestgaard, B.G.; Andersen, T.; Sorensen, T.I.; Lange, P. Body mass, fat-free body mass, and prognosis in patients with chronic obstructive pulmonary disease from a random population sample: Findings from the Copenhagen City Heart Study. Am. J. Respir. Crit. Care Med. 2006, 173, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Reumatologie, N.V.v. Richtlijn osteoporose en fractuurpreventie, 3e herziening. In Hoofdstuk 8: Diagnostiek en Behandeling van Osteoporose bij Mannen; NVR: Utrecht, The Netherlands, 2011. [Google Scholar]
- Kdoqi. KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Diabetes and Chronic Kidney Disease. Am. J. Kidney Dis. 2007, 49, S12–S154. [Google Scholar] [CrossRef] [PubMed] [Green Version]





| COPD | Controls | |
|---|---|---|
| Number of subjects, n | 208 | 200 |
| Male, n (%) | 58 | 45 1 |
| Age, years | 62 ± 7 | 61 ± 7 1 |
| BMI, kg/m2 | 26.9 ± 5.4 | 26.9 ± 3.4 |
| Former smoker, % | 65 | 55 1 |
| Current smoker, % | 34 | 11 1 |
| Pack-years, n | 43 (29–58) | 6 (0–20) 1 |
| Fram.10-yr. risk ≥ 30%, % | 32 | 19 1 |
| FEV1, % predicted | 50 ± 16 | 119 ± 15 1 |
| FEV1/FVC | 41 ± 12 | 79 ± 5 1 |
| ITGV, % predicted | 144 ± 33 | 100 ± 18 1 |
| KCO, % predicted | 69 ± 22 | 101 ± 16 1 |
| MRC dyspnea grade | 3.0 ± 1.0 | NA |
| SGRQ, total score | 55.0 ± 16.5 | NA |
| 6MWD, m | 458 ± 131 | NA |
| ≥2 ex. previous year, n (%) | 45 | NA |
| Telomere length, kbp | 10.37 ± 1.78 | 10.94 ± 1.47 1 |
| C1 | C2 | C3 | C4 | C5 | |
|---|---|---|---|---|---|
| Cluster description | Less Comorbidity | Cardiovascular | Metabolic | Psychologic | Cachectic |
| Subjects, n (%) | 46 (22%) | 27 (13%) | 56 (27%) | 40 (19%) | 39 (19%) |
| Comorbidities, n | 2.5 ± 1.2 1 | 3.4 ± 0.9 | 5.0 ± 1.3 1 | 4.8 ± 1.9 1 | 3.4 ± 1.4 1 |
| Hypertension, % | 20 1 | 96 1 | 86 1 | 55 | 28 1 |
| Arterial Stiffness, % | 27 1 | 92 1 | 78 1 | 53 | 29 1 |
| Atherosclerosis, % | 33 | 16 | 47 1 | 42 | 6 1 |
| Hyperglycemia, % | 80 | 48 1 | 82 1 | 67 | 54 1 |
| Insulin resistance, % | 5 1 | 0 1 | 52 1 | 11 | 0 1 |
| Obesity, % | 28 | 22 | 54 1 | 25 | 0 1 |
| Dyslipidemia, % | 26 | 0 1 | 79 1 | 44 | 15 1 |
| Renal Impairment, % | 22 | 22 | 14 | 28 1 | 3 1 |
| Osteoporosis, % | 7 | 33 1 | 7 | 15 | 24 |
| Low muscle mass, % | 0 1 | 11 | 6 1 | 3 1 | 80 1 |
| Underweight, % | 0 1 | 0 1 | 0 1 | 5 1 | 80 1 |
| Anxiety, % | 2 1 | 8 1 | 9 1 | 95 1 | 14 |
| Depression, % | 9 | 0 1 | 9 1 | 59 1 | 14 |
| C1 | C2 | C3 | C4 | C5 | |
|---|---|---|---|---|---|
| Cluster description | Less Comorbidity | Cardiovascular | Metabolic | Psychologic | Cachectic |
| Subjects, n (%) | 46 (22%) | 27 (13%) | 56 (27%) | 40 (19%) | 39 (19%) |
| Male, % | 63 | 67 | 64 | 43 1 | 51 |
| Age, years | 61 ± 7 | 65 ± 7 1 | 64 ± 6 | 61 ± 8 | 60 ± 6 |
| BMI, kg/m2 | 27.2 ± 4.0 | 26.9 ± 3.5 | 31.1 ± 4.9 1 | 27.5 ± 3.8 | 19.9 ± 2.0 1 |
| Waist circumference, cm | 102 ± 12 | 102 ± 12 1 | 112 ± 14 | 102 ± 15 | 82 ± 8 1 |
| Former smoker, % | 59 | 89 1 | 75 | 58 | 49 1 |
| Current smoker, % | 39 | 11 1 | 26 | 40 | 49 1 |
| Pack-years, n | 39 (27–45) 1 | 40 (27–45) | 45 (32–57) | 58 (31–84) 1 | 43 (28–59) |
| Fram.10yr. risk ≥ 30%, % | 18 1 | 37 | 60 1 | 26 | 10 1 |
| FEV1, % predicted | 51 ± 16 | 49 ± 16 | 56 ± 13 1 | 48 ± 15 | 40 ± 15 1 |
| FEV1/FVC | 41 ± 12 | 40 ± 10 | 46 ± 11 1 | 40 ± 11 | 36 ± 12 1 |
| ITGV, % predicted | 139 ± 28 | 149 ± 30 | 128 ± 30 1 | 144 ± 30 | 171 ± 32 1 |
| KCO, % predicted | 67 ± 22 | 68 ± 17 | 80 ± 24 1 | 66 ± 18 | 58 ± 18 1 |
| MRC dyspnea grade | 3.0 ± 0.8 | 2.9 ± 1.1 | 2.9 ± 1.2 | 3.2 ± 0.9 | 3.0 ± 1.1 |
| SGRQ, total score | 48.3 ± 15.0 1 | 56.1 ± 18.7 | 53.6 ± 15.1 | 66.2 ± 13.7 1 | 52.2 ± 16.2 |
| 6MWD, m | 445 ± 168 | 450 ± 159 | 462 ± 121 | 466 ± 100 | 465 ± 116 |
| ≥2 ex. previous year, % | 46 | 33 | 44 | 48 | 53 |
| X1 | X2 | X3 | |
|---|---|---|---|
| Cluster description | Less (Co)morbidity | Cardiovascular | Metabolic |
| Subjects, n (%) | 97 (49%) | 34 (17%) | 69 (35%) |
| Comorbidities, n | 1.4 ± 1.0 1,2 | 3.8 ± 0.8 1 | 3.1 ± 1.3 1,2 |
| Hypertension, % | 44 1,2 | 100 1 | 462 |
| Arterial Stiffness, % | 1 1,2 | 100 1 | 5 1,2 |
| Atherosclerosis, % | 17 1,2 | 28 | 32 |
| Hyperglycemia, % | 46 1,2 | 68 | 74 1 |
| Insulin resistance % | 1 1 | 0 | 19 1,2 |
| Obesity, % | 0 1,2 | 21 | 36 1 |
| Dyslipidemia, % | 0 1,2 | 35 2 | 78 1 |
| Renal Impairment, % | 4 2 | 12 | 10 |
| Osteoporosis, % | 9 | 6 2 | 3 |
| Low muscle mass % | 7 | 6 | 3 |
| Underweight, % | 5 | 3 | 0 |
| Anxiety, % | 1 | 3 | 4 |
| Depression, % | 1 2 | 0 | 3 |
| X1 | X2 | X3 | |
|---|---|---|---|
| Cluster description | Less (co)morbidity | Cardiovascular | Metabolic |
| Subjects, n (%) | 97 (49%) | 34 (17%) | 69 (35%) |
| Comorbidities, n | 1.4 ± 1.0 1,2 | 3.8 ± 0.8 1 | 3.1 ± 1.3 1,2 |
| Male, % | 34 1,2 | 59 | 54 |
| Age, years | 60 ± 6 1 | 66 ± 6 1 | 60 ± 6 2 |
| BMI, kg/m2 | 25.4 ± 2.4 1,2 | 27.4 ± 3.8 | 28.7 ± 3.5 1,2 |
| Waist circumference, cm | 89 ± 10 1,2 | 95 ± 10 2 | 98 ± 11 1,2 |
| Former smoker, % | 53 | 62 2 | 54 2 |
| Current smoker, % | 8 2 | 9 | 15 |
| Pack-years, n | 5 (0–16) 1,2 | 5 (0–22) 2 | 10 (0–25) 1,2 |
| Fram.10yr. risk ≥30%, % | 9 1 | 33 1 | 29 1,2 |
| FEV1, % predicted | 119 ± 15 2 | 122 ± 16 2 | 118 ± 15 2 |
| FEV1/FVC | 78 ± 5 2 | 78 ± 5 2 | 79 ± 5 2 |
| ITGV, % predicted | 106 ± 20 1,2 | 98 ± 17 2 | 94 ± 14 1,2 |
| KCO, % predicted | 99 ± 15 2 | 100 ± 14 2 | 105 ± 18 1,2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triest, F.J.J.; Franssen, F.M.E.; Reynaert, N.; Gaffron, S.; Spruit, M.A.; Janssen, D.J.A.; Rutten, E.P.A.; Wouters, E.F.M.; Vanfleteren, L.E.G.W. Disease-Specific Comorbidity Clusters in COPD and Accelerated Aging. J. Clin. Med. 2019, 8, 511. https://doi.org/10.3390/jcm8040511
Triest FJJ, Franssen FME, Reynaert N, Gaffron S, Spruit MA, Janssen DJA, Rutten EPA, Wouters EFM, Vanfleteren LEGW. Disease-Specific Comorbidity Clusters in COPD and Accelerated Aging. Journal of Clinical Medicine. 2019; 8(4):511. https://doi.org/10.3390/jcm8040511
Chicago/Turabian StyleTriest, Filip J. J., Frits M. E. Franssen, Niki Reynaert, Swetlana Gaffron, Martijn A. Spruit, Daisy J. A. Janssen, Erica P. A. Rutten, Emiel F. M. Wouters, and Lowie E. G. W. Vanfleteren. 2019. "Disease-Specific Comorbidity Clusters in COPD and Accelerated Aging" Journal of Clinical Medicine 8, no. 4: 511. https://doi.org/10.3390/jcm8040511